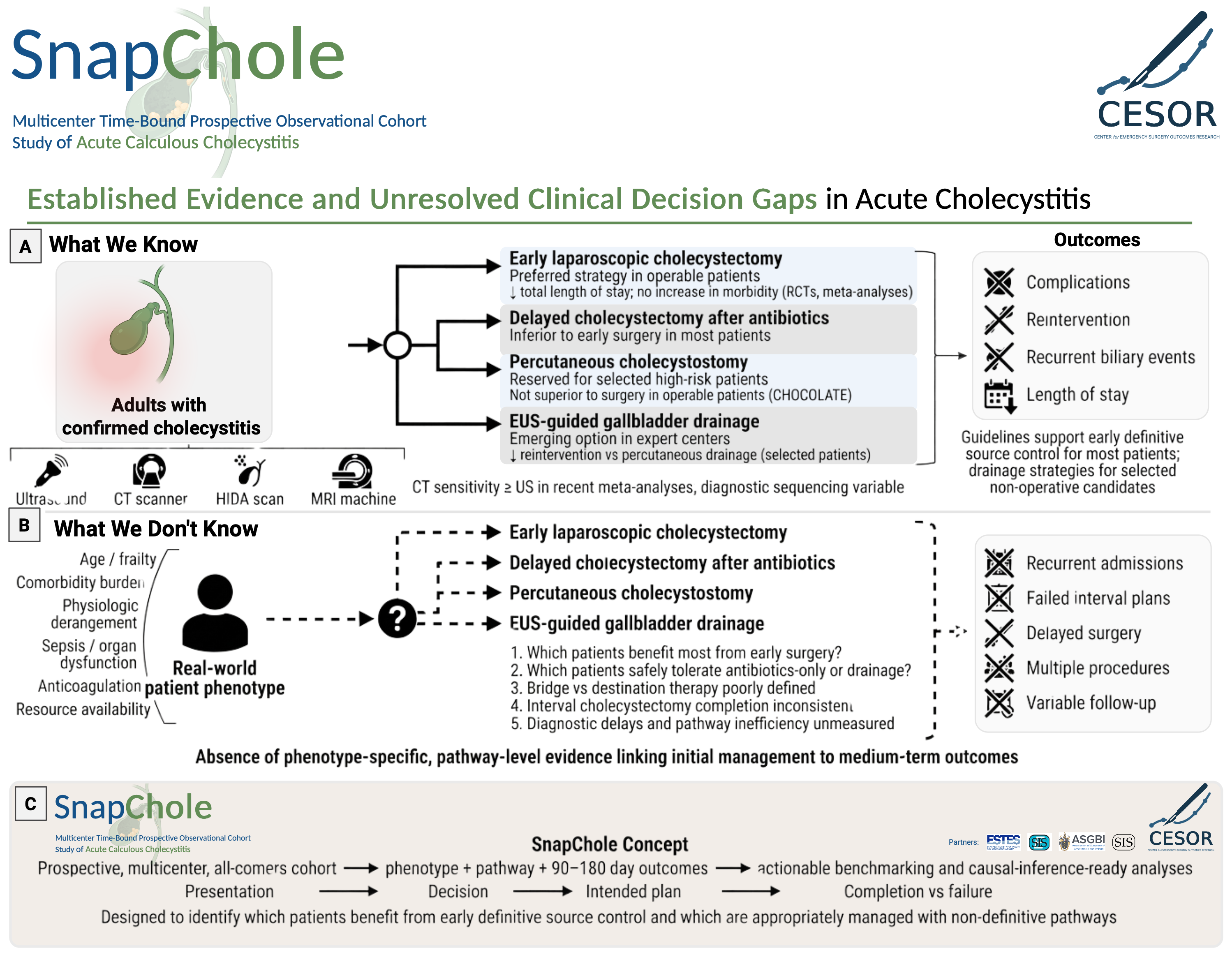
Acute calculous cholecystitis is common, but severe disease is where strategy selection becomes most consequential. Patients may be assigned to early cholecystectomy, drainage-first, or antimicrobial-only management under superficially similar decision contexts, yet those decisions are shaped by physiologic reserve, reversibility of organ dysfunction, diagnostic certainty, and system capability.
SnapChole addresses that problem. The study does not treat pathway selection as a retrospective coding exercise. It captures the attending surgeon–level decision point as time zero and preserves the variables needed to estimate the effect of source-control strategies in clinically coherent populations.